What’s the correct painkiller prescription to ship house with a affected person after gallbladder surgical procedure or a cesarean part?
That query is entrance and middle as standard approaches to ache management within the United States have led to what some see as a tradition of overprescribing, serving to spur the nation’s epidemic of opioid overuse and abuse.
The reply isn’t clear-cut.
Surgeon Marty Makary questioned why and what could possibly be completed.
So, Makary, a researcher and a professor of surgical procedure and well being coverage at Johns Hopkins School of Medicine in Baltimore, took an progressive strategy towards creating tips: matching the correct variety of opioid painkillers to particular procedures.
After all, most docs normally make this determination primarily based on one-size-fits-all suggestions, or what they discovered way back in med faculty.
Even Makary admitted that for many of his profession he “gave [painkillers] out like candy.”
In December, he gathered a bunch of surgeons, nurses, sufferers and different leaders, asking them: What ought to we be prescribing for operation X?”
The reply was illuminating.
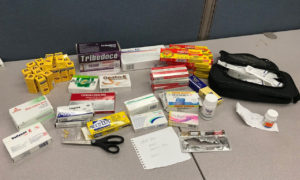
“No one should have 50 tabs sitting in their medicine cabinet” for acute ache, says Dr. Marty Makary, who’s main an effort to curb overprescribing by providing procedure-specific tips for opioid painkillers. (Courtesy of Johns Hopkins Medicine)
“The head of the hospital’s pain services said, ‘You’re the surgeon, what do you think?’” recalled Makary.
Makary didn’t know. Nor did the resident. And the nurse practitioner, who usually is the one who most carefully follows up with sufferers, stated it varies.
“Wow,” remembers Makary of that day after they first thought of acceptable limits. “We’re the experts, the heads of this and that, and we don’t know.”
After a fast couple of weeks of intense dialogue, Makary’s group reached consensus and gave its blessing to guidelines setting maximum numbers of opioid-containing drugs for 20 totally different widespread surgical conditions, from comparatively minor procedures to coronary bypass surgical procedure.
“We’re in a crisis,” stated Makary, explaining why the group didn’t go a extra conventional route and publish its findings in a medical journal first, which may take months.
Sometimes the correct variety of opioids is zero, concluded the group.
Indeed, it recommends no opioids for sufferers heading house after uncomplicated labor and supply, or after cardiac catheterization, a process during which a skinny, hole tube is inserted into the guts via a blood vessel to test for blockages.
For sure sorts of knee surgical procedure, corresponding to arthroscopic meniscectomy, the rules suggest not more than 12 drugs upon discharge, whereas a affected person going house after an open hysterectomy may require as many as 20.
Optimally, “no one should be given more than five or 10 opioid tablets after a cesarean section,” Makary stated.
Oh, and for cardiac bypass surgical procedure? No greater than 30 drugs.
Email Sign-Up
Subscribe to KHN’s free Morning Briefing.
But What About The Pain?
Tens of hundreds of Americans are dependent upon opioid drugs. An rising quantity are dying from overdoses, each from prescription treatment and road medicine.
Knowing that, Makary, in addition to different surgeons, hospitals and organizations, are taking steps to vary how they follow medication.
After all, many consultants view using opioid prescription painkillers after surgical procedure as a gateway to long-term use or dependence. A study printed final 12 months within the journal JAMA Surgery discovered that persistent use of opioids was “one of the most common complications after elective surgery.”
In that research, University of Michigan researchers discovered that 6 % of people that had by no means taken opioids however obtained them after surgical procedure had been nonetheless taking the drugs three to 6 months later.
With about 50 million surgical procedures that happen within the U.S. annually, “there are millions who may become newly dependent,” stated Chad Brummett, the research’s lead writer and an affiliate professor of anesthesiology on the University of Michigan Medical School.
Smokers, and people recognized with sure circumstances corresponding to melancholy, anxiousness or persistent ache earlier than their operations, had been most liable to long-term use.
Each refill or extra week of use makes for a better danger of misuse, different studies have proven.
Additional analysis factors to a different cause for concern. If sufferers don’t take all of the drugs they’re prescribed following an operation, these drugs may be stolen or diverted to different individuals, who then run the danger of turning into dependent.
Still, there’s debate in medical circles about simply how efficient suggestions and tips might be in stemming the epidemic.
For one factor, some consultants fear that if the struggle towards opioids focuses solely on protected prescribing on the expense of in search of alternate options, it might miss the larger image.
“Are there better methods than opioids in the first place?” asks Lewis Nelson, chair of emergency medication at Rutgers New Jersey Medical School. “Could you put a lidocaine patch over the wound or is there a better way to immobilize a joint?”
Studies have shown that typically a mix of ibuprofen and acetaminophen may be simply nearly as good as or higher than opioids.
Alternatives ought to all the time be thought of first, agreed Makary.
Another concern is that tips for prescribing reduction — even these aimed toward short-duration, acute ache, corresponding to that following surgical procedure — have carryover results on sufferers with long-term ache. Advocates say all the eye round prescribing limits have made it troublesome for persistent ache sufferers to get the drugs they want.
Some individuals even apply these considerations to suggestions in regards to the remedy of acute ache.
“It’s important for a physician to have the ability, if they feel there’s a medical necessity, to write a prescription for a longer duration,” stated Steven Santos, president of the American Academy of Pain Medicine. “It’s challenging to lump all patients into one basket.”
A Different Focus: Duration
Lawmakers — determined to deal with overdose issues which can be destroying households and communities — have gone the place they normally don’t: setting particular guidelines for docs.
Legislatures in additional than a dozen states, together with New Jersey, Massachusetts and New York, have set restrictions, usually on the variety of days’ price of drugs prescribed for acute ache.
“States said that since physicians haven’t self-regulated, we’re going to do it for them,” stated Nelson at Rutgers.
Congress, too, is getting concerned, holding a flurry of hearings this spring, and contemplating laws that might, amongst different issues, set limits on prescribing opioids for acute ache. The just lately handed federal spending invoice consists of $three billion in new funding to assist states and native governments with opioid prevention, remedy and regulation enforcement efforts.
To be certain, the medical career has additionally responded to the disaster — with medical societies and different knowledgeable teams providing a rising variety of requirements for prescribing opioids.
Some are pretty generic, recommending the bottom dose for the shortest time frame for acute ache. Some are extra prescriptive.
None is supposed to deal with the wants of persistent ache sufferers or these with most cancers.
And state guidelines range. New Jersey’s, for instance, says sufferers with acute ache ought to, initially, get not more than a five-day provide, whereas Massachusetts units the cap at seven days for a affected person prescribed opiates for the primary time.
The Centers for Disease Control and Prevention recommends three days.
Makary and another consultants say that, whereas well-intentioned, such durational guidelines are too blunt.
A day’s price of drugs can range, relying on how usually the physician instructs sufferers to take them. Under lots of the state guidelines, sufferers may nonetheless head house with greater than 50 drugs.
“No one should have 50 tabs sitting in their medicine cabinet” for acute ache, stated Makary.
Andrew Kolodny, co-director of opioid coverage analysis on the Heller School for Social Policy and Management, helps tips however needs states to take their guidelines a step additional.
“I don’t think the way the states are going at this makes much sense because the issue with overprescribing was quantity, yet they’re passing laws around duration,” he stated.
Instead, the legal guidelines ought to require that “if physicians are going to prescribe more than three days, they have to warn the patients that this is an addictive drug and that taking it every day for as little as five days may cause them to become physiologically dependent,” Kolodny stated.
That would create a disincentive to prescribing greater than three days’ price of opioid painkillers, he added, and result in extra knowledgeable sufferers amongst those that want an extended provide.
Rutgers’ Nelson, who sat on the CDC panel that developed suggestions, stated durational guidelines — like these adopted by the states — may be efficient.
“I personally think three days is enough,” stated Nelson. “That doesn’t mean pain goes away in three days, but most people get better within three to five days.”
That stated, Nelson known as the Hopkins’ strategy an “excellent idea” and one he has tried to do. “It’s a lot harder than it sounds because of the large number of procedures and the diversity of patient needs,” he stated.
To get round overprescribing — or setting one-size-fits-all tips — physicians at Dartmouth-Hitchcock Medical Center have a developed their very own data-based strategy.
Dr. Richard Barth, the chief of normal surgical procedure at Dartmouth, and colleagues studied 333 sufferers discharged from the hospital following six widespread surgical procedures that included bariatric procedures; operations on the abdomen, liver, colon and pancreas; and hernia restore.
Surveying the sufferers, they requested what number of opioid drugs they went house with, what number of they really took, what number of went unused and the way a lot ache they skilled.
The information helped them land on a strategy to suggest a selected variety of drugs. “If they took none the day before discharge, then over 85 percent of patients did not take any when they went home,” stated Barth.
Dartmouth-Hitchcock now makes use of that information as a really useful start line for physicians.
Under the guidelines, sufferers taking no opioid ache drugs the day earlier than discharge go house with none. Those who take one to 3 drugs get 15, an quantity Barth’s research discovered glad 85 % of sufferers, and people who took 4 or extra get 30 drugs.
“We came out with a very easy to implement and remember guideline,” stated Barth. “We actually called patients and asked them how many [pills] they used. That’s what differentiates us from other places.”
Brummett, at Michigan, says the Opioid Prescribing Engagement Network, a collaboration of hospitals, insurers, physicians and others in his state, has used comparable information strategies to give you procedure-specific tips.
“We’ve taken a data-driven approach,” he stated. “We believe patient-reported outcomes are a better way to guide than expert consensus.”
For his half, Makary admitted it’s more durable to develop tips like these at Hopkins and Dartmouth, however he stated the hassle is significant.
“It’s mind-boggling to me” that so many opioid-prescribing tips don’t specify the process, stated Makary. “An ingrown toenail is not the same as cardiac bypass surgery.”
Julie Appleby: [email protected]”>[email protected], @Julie_Appleby
Related Topics Health Industry Public Health States Doctors Hospitals Legislation Nurses Opioids Prescription Drugs Substance Abuse src=”http://platform.twitter.com/widgets.js” charset=”utf-Eight”>