A person stands outdoors Dr. Sunil Sagar’s clinic, which caters to residents of Bhagwanpur Khera.
This story is the second in a two-part collection. Read half one right here: “In India’s Slums, Painkillers Part Of Daily Routine.”
NEW DELHI — In the crowded ready room of Dr. Sunil Sagar’s clinic, within the working-class neighborhood of Bhagwanpur Khera, a toddler breathes from a nebulizer. Fever is widespread, and the air high quality in Delhi has reached “severe-plus emergency.” The sufferers sit, immobile, however there’s someway great noise. The clinic is a squat cement constructing draped in wires, a purple cross on the door. Sagar sits behind a desk in a small, open room, as a squad of assistants escort sufferers to him. He appears totally unflappable.
A father with a troubled look sits down subsequent to the physician, holding a child. Sagar listens to the infant’s chest with a stethoscope, pulls out scrap paper and writes a prescription. The father palms over a number of rupees, and Sagar locations the payments right into a cash drawer beneath his desk. The total change takes maybe two minutes.
Medicine in India is transactional. A popular physician palms over a prescription on the finish of each go to. Why else have I paid money to see the physician, if not for aid? The precariousness of every day life leaves little room for downtime.
As the Indian authorities reluctantly loosens its prescription opioid legal guidelines after a long time of lobbying by palliative care advocates determined to ease their sufferers’ acute ache, the nation’s sprawling, cash-fed well being care system is ripe for misuse. The sheer measurement of India’s system — tens of tens of millions of medical doctors and pharmacies unfold throughout the subcontinent — makes oversight troublesome however presents a tantalizing alternative for India’s burgeoning ache business and multinational pharmaceutical firms looking for new markets.
A preferred spot to buy these bulk medication is the Bhagirath Palace within the Chandni Chowk market, one among India’s largest wholesale markets that dates to the 17th century. It is a dense maze the place males — and it nearly fully males — press their our bodies right into a present of economic ecstasy, continuously thrown off track by honking auto rickshaw drivers. One after the following, stalls of drug distributors promote on brightly painted indicators “all types of medicines,” “life-saving anti-cancer drugs,” “deal in Glaxo … Johnson & Johnson.” Inside the stalls, packing containers of drugs are stacked from flooring to ceiling.
Dr. Sunil Sagar checks medicines after he examines a affected person at his clinic. (Saumya Khandelwal/The Guardian)
An outdoors view from Dr. Sunil Sagar’s clinic.(Saumya Khandelwal/The Guardian)
One drug wholesaler out there stated the federal government has been cracking down currently on sure medicines. Recently, he had obtained an inventory of 328 medication that he was not alleged to inventory, together with Sulpitac, an antipsychotic medicine used to deal with schizophrenia. The wholesaler stated folks had been taking it like “dal and rice” for complications.
Like its inflexible caste system, India’s ache business is stratified. The well-to-do go to well-appointed ache clinics, the working class flip to their neighborhood medical doctors, and the decrease castes, particularly these residing in India’s huge slums, scramble for aid at roadside pharmacies, referred to as chemists.
In the Mankhurd slum in Mumbai, the place the common life expectancy is 39, toddlers wander bare-bottomed, defecating on the street. Children scratch at infections on their legs. Without any municipal water, hawkers promote plastic sandwich luggage stuffed with soiled water for two rupees. In this place, ache cures are available.
At Shiv Medical & General Stores, an older boy tending the stall wrote out a receipt for Ultracet, branded tramadol tablets — an opioid analgesic — made by a Johnson & Johnson subsidiary. “Doctor’s name?” he requested. Our information, Mayur Helia, a neighborhood organizer, made one up. “Shagmu,” Helia stated, laughing, and the shopkeeper wrote it down.
Helia and his colleagues are activists agitating for consuming water and sanitation within the Mumbai-area slums. “Painkillers are part of the daily routine,” stated social employee Alfiya Mulla. “They have become more normalized.”
“You go to the chemist,” Helia added, “and you say, ‘I have this pain,’ and he will give you painkillers without any prescription.”
Daily life here’s a pageant of hustle. For ladies within the slums, Mulla stated, which means lugging 35-liter buckets of water. “You have to take that from half a kilometer away, and that’s why women have to take that” — she motioned to the field of Ultracet — “because they are hurting their backs.”
She turned the field over in her palms. “Women are more affected and are more addicted to this tablet.”
Shopkeepers work inside a pharmacy store on the Bhagirath Palace prescribed drugs market in Old Delhi.
Beautiful Laws, Lax Enforcement
As India flirts with liberalizing entry to painkillers, authorities surveys present dependancy to prescription opioids is on the rise. The northern state of Punjab, the place heroin dependancy is endemic, not too long ago opened greater than 160 outpatient opioid-assisted remedy clinics the place addicts can obtain substitute opioids like buprenorphine whereas they battle withdrawal.
But buprenorphine can be broadly prescribed to deal with persistent ache and has change into an issue in its personal proper. Dr. Debasish Basu, a psychiatrist and professor on the Postgraduate Institute of Medical Education and Research in Chandigarh, one among India’s high medical institutes, stated “the main prescription medicine that we’re seeing [people becoming addicted to] is buprenorphine.”
“The source for buprenorphine is a licit source; they are made in drug-manufacturing factories,” he stated, however then “the diversion takes place.”
Basu echoed well being consultants throughout the nation in saying the central authorities tightly regulates the manufacturing of narcotic painkillers, however there’s little religion in its capability to regulate distribution. “The legal system is so lax, the monitoring system is so lax,” Basu lamented. “The laws are all there. Oh, there are beautiful laws. But the implementation is so lax that once something comes over here, it’s very difficult. It’s like a bonfire.”
A affected person enters Dr. Sunil Sagar’s workplace at his clinic.
If there’s a precursor to an American-style opioid epidemic in India, it’s tramadol, a painkiller that grew to become obtainable right here within the early 1990s. Drugmakers — typically citing research that they had funded — touted tramadol as much less addictive than different painkillers.
“Tramadol information would come to every single clinician,” stated Dr. Bobby John, a Delhi-based well being professional. “Why? Because there is some drug salesperson sitting outside your door saying, ‘Hey, there’s a new drug. It’s non-addictive.’ Standard playbook.”
Tramadol flourished in India. Unlike morphine, fentanyl and different painkillers, the federal government initially positioned few restrictions on its sale. But in 2018, after studies of abuse within the state of Punjab and studies of illicit Indian tramadol being bought to Boko Haram militants in Nigeria and elsewhere in Africa, Indian regulators enacted stricter controls.
If you can not see the direct affect of American pharmaceutical firms in India, you may detect their shadow. In October 2018, simply months after the Indian authorities clamped down on tramadol, a gaggle of ache specialists from seven Southeast Asian international locations, together with three from influential hospitals in India, printed a paper within the Journal of Pain Research.
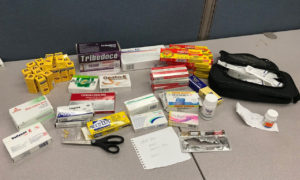
Loose capsules at Dr. Sagar’s clinic dispensary.
“Tramadol: A Valuable Treatment for Pain in Southeast Asian Countries” made the case that “the weak opioid tramadol has become the analgesic most frequently used in the region to treat moderate to severe pain.” The paper concluded: “If it were to become a controlled substance, the standard of pain management in the region would decline.”
The paper was funded by Grünenthal GmbH of Germany, an organization that signed a deal in May 2018 to permit Mundipharma to market and distribute its tramadol product, Tramal, in China. Authors included ache specialists who’ve obtained consulting and lecturing charges from Pfizer, Johnson & Johnson and Mundipharma, a community of firms managed by the Sackler household, homeowners of Connecticut-based Purdue Pharma.
Dr. Pooja Garg runs an opioid-assisted dependancy restoration clinic on the outskirts of Chandigarh, one among 5 within the space. Addicts within the space favor heroin, she stated, however after they can’t discover or afford heroin, “they take whatever they can get over the counter from chemists.” That tends to be tramadol, which, regardless of the brand new restrictions, stays broadly obtainable.
The bustling ready room led right into a peaceable internal courtyard the place, on a weekday morning final November, dozens of younger males, of their late teenagers and 20s, had come for inpatient remedy. In one bed room, a number of males sat cross-legged on a pair of metallic cots. The younger males stated they took tramadol or buprenorphine, no matter they may get. “It depends on the availability at that particular moment,” one stated. They all agreed tramadol was straightforward to purchase from native chemists.
India sits between the 2 largest illicit opium-growing areas, the Golden Crescent of Afghanistan, Iran and Pakistan, and the Golden Triangle of Laos, Myanmar and Thailand; and India itself is without doubt one of the largest producers of authorized opium. Much of the heroin passes via Punjab, a state of 28 million in northwestern India that has struggled with opioid dependancy.
That historical past of heroin dependancy makes these in Punjab and different close by states particularly weak to artificial opioids, stated Dr. Anshu Garg, an dependancy counselor in Mohali. Heroin “is freely available in the villages,” he stated. “People try it without knowing the consequences. They try it once or twice, they get addicted to it.”
A pharmacy store in Bhagwanpur Khera, New Delhi.
Sharing The Spoils
Vijay Bhatia can attest to how the enterprise acumen propelling India towards financial prosperity has been overtly co-opted by keen pharmaceutical firms.
Bhatia labored in pharmaceutical gross sales for twenty years for a handful of firms, together with GlaxoSmithKline and Ranbaxy Laboratories, an Indian generics maker owned by Sun Pharma. He now works in Chandigarh, the place he oversees gross sales for Atulaya Healthcare, a series of diagnostic imaging facilities. Bhatia was amongst a number of present or former pharma representatives interviewed who described how multinational drugmakers deploy refined strategies in India for getting their merchandise prescribed.
Drugmakers routinely give gross sales representatives extra cash to supply medical doctors money or items — iPads, automobiles, journeys to conferences — to prescribe the drug they’re promoting, Bhatia stated. He described how gross sales reps give influential medical doctors free merchandise to check with sufferers and the way some medical doctors, in flip, ship lectures at all-expenses-paid symposia, typically presenting analysis papers sponsored by the drug firms.
The multinational firms “have access to all these top opinion leaders,” Bhatia stated. They will sponsor medical doctors to dwell “abroad for studies being done there. It is circumventing the entire marketing process. It’s another way of taking the doctor into the loop.”
“Suppose a product costs $100. To the company, it is costing $20. Now they have $80 to play with,” Bhatia defined. “So they’ll keep a safe margin, say, ‘OK, fine, this much money you can keep for ongoing practices or for sponsoring the doctor or, right or wrong, bribing the doctor.’”
Engendering loyalty with chemists is a high precedence. To make his gross sales targets, Bhatia stated, he would supply monetary incentives to chemists who would “substitute [a product] with my product. In India, the chemist becomes king.”
Multinational pharmaceutical firms preserve they’re moral purveyors of their merchandise. “Opioid pain medications play an essential role in the management of severe pain and it’s important they be recognized by health authorities as important therapeutic options, especially in cancer pain,” Manmohan Singh, a vp at Modi-Mundipharma in New Delhi, stated in a written assertion. But, he stated, “they need to be appropriately prescribed, monitored and reviewed to minimize the risks of misuse and abuse.”
In all gross sales promotions, Singh stated, his firm stresses that sufferers must be rigorously chosen, prescribed the bottom efficient dosage, and made conscious of each the remedy targets and potential uncomfortable side effects. “The exact prevalence of addiction with opioids is difficult to determine,” he stated. “Signs of addictive behavior should be monitored and addressed.”
A girl seems to be out from a balcony of a home close to Sagar’s clinic, which caters to residents of Bhagwanpur Khera.
In Thiruvananthapuram, within the southern state of Kerala, Dr. M.R. Rajagopal is aware of all too properly highly effective drug firm, a grasping pharmaceutical salesman, an unscrupulous ache physician, a reckless morphine addict or any whiff of scandal someplace on the subcontinent may sink his life’s work. Widely considered as the daddy of palliative care right here, he’s frankly uninterested in “opiophobia,” the “prejudice and misinformation” that the medical use of opioids will result in dependancy and crime. He is uninterested in reassuring Indian bureaucrats they aren’t ushering in a U.S.-style opioid epidemic. He has no time for doomsday situations; there are too many Indians in agony.
“This is a rather horrible country to die in,” Rajagopal instructed a roomful of medical doctors and medical college students final fall at Sree Gokulam Medical College, on the outskirts of Thiruvananthapuram. He stood unassumingly on the entrance of a hospital convention room darkened by thick purple drapes. Even with a microphone, his voice was light. “If a patient cries in pain for two weeks” on the finish of his life, Rajagopal stated, “it is hard to remember any good times.” When they’re dying, he urged the gang, “Give morphine.”
Despite the blossoming ache business, Rajagopal estimates not more than 2% of Indians have entry to palliative care. In his testimony for a three-year examine of untreated ache printed by the Lancet medical journal in 2018, he recounted the story of “Mr. S,” who got here to a palliative care clinic in Calicut, Kerala, with crippling ache from lung most cancers. He put the person on morphine, and some hours later, Mr. S “surveyed himself with disbelief. He had neither hoped nor conceived of the possibility that this kind of relief was possible.”
When Mr. S returned the next month, the clinic had run out of morphine. The affected person “instructed us with outward calm, ‘I shall come again next Wednesday. I will bring a piece of rope with me. If the tablets are still not here, I am going to hang myself from that tree.’
“He pointed to the window. I believed he meant what he stated.”
Read half one among this two-part collection: “Beset By Lawsuits And Criticism In U.S., Opioid Makers Eye New Market In India“